Pancreatic Surgery
Airway: ETT
Access: 14G and CVC
Pain: Substantial, use ITM or thoracic epidural
Position: Supine
Time: 4-8 hours
Blood loss: 0.5-1.5L
Special: NG tube, neuraxial analgesia
The Bottom Line:
- Major surgery typically occurring in an older cohort with malignant cachexia
- Typically late presentation limiting opportunity for prehabilitation
- Potential for endocrinologically active tumours requiring close intraoperative BSL monitoring
- Significant analgesia requirements
Pancreatic surgery can include resection of the:
The pancreas has complex anatomy necessitating complex resection:
- Two embryological buds (head and tail) with dual blood supply
- Head and uncinate process share perfusion with duodenum (via SMA)
- Body and tail supplied by splenic artery (via coeliac trunk)
- May be incompletely fused, leading to separate ducts into the duodenum
- Extensive anatomical variability with variable arterial dominance
- Pancreatic head
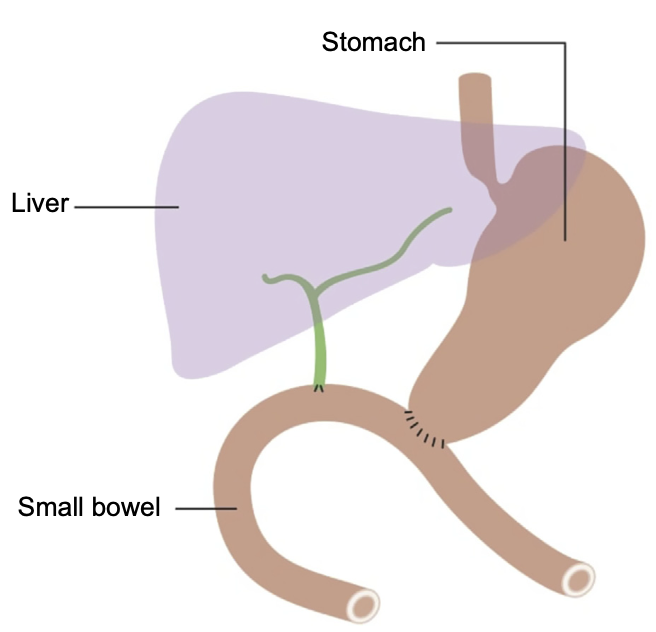
Two broad approaches:- The “Classic Whipple”
- Resection of head of pancreas, gallbladder, duodenum, distal stomach, lower common hepatic duct
- Three anastomoses:
- Pancreaticojejunostomy
- Hepaticojejunostomy
- Gastrojejunostomy
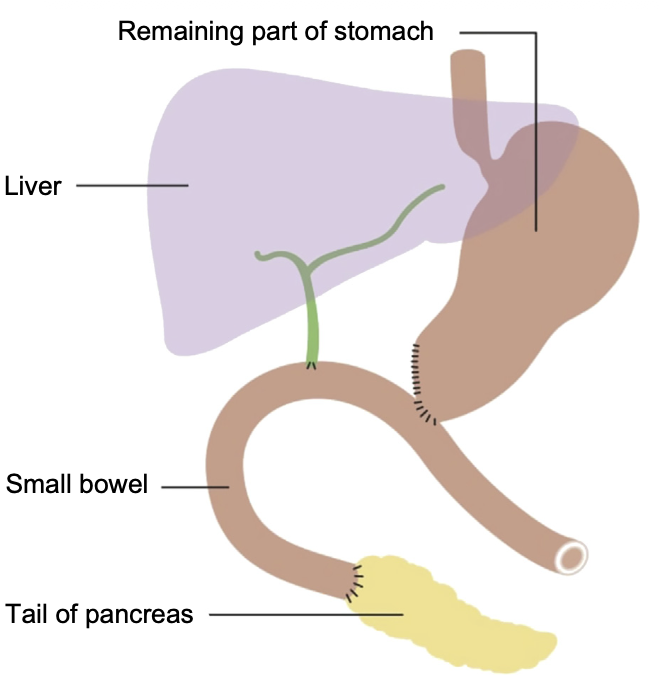
- Pylorus-preserving
Improve nutrition, ↓ gastric dumping, and ↓ jejunal ulceration:- Pylorus-preserving pancreaticoduodenectomy
- Pylorus and distal stomach preserved
- Gastrojejunostomy becomes duodenojejunostomy
- Pylorus-resecting pancreaticoduodenectomy
Less distal stomach resection than a a Whipple.
- Pylorus-preserving pancreaticoduodenectomy
- The “Classic Whipple”
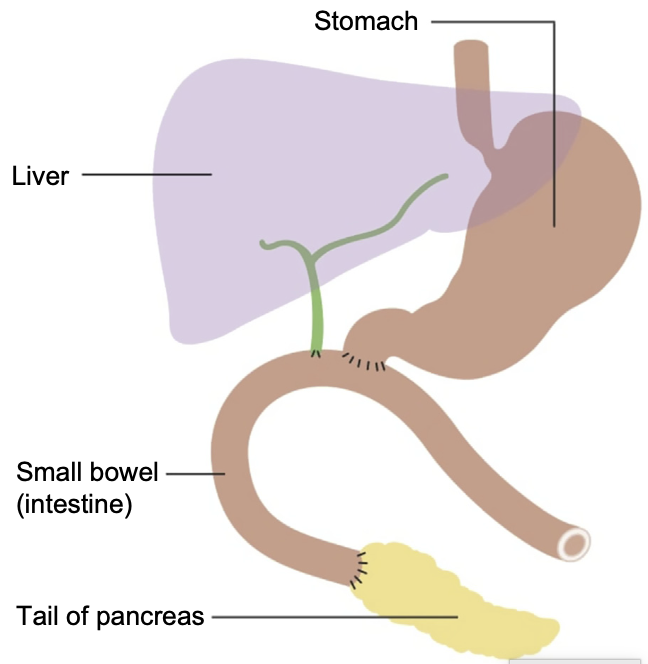
- Distal pancreas
- Significantly reduces operative complexity
No anastomoses required, as duodenum, stomach, and biliary tree are unaffected. - Splenic preservation may be possible depending on the anatomy
- Significantly reduces operative complexity
- Total pancreatectomy
- Requires anastomoses of pancreatic head resection, and en bloc splenectomy
- Complex post-operative diabetes
Pancreatic malignancy can be split into:
- >95% ductal adenocarcinoma
- <5% Endocrine tumours
Islet cell and pluripotent epithelial tumours. May be:- Non-functioning
- Functioning
Hormone producing (~10-30%). Include:- Insulinomas
- ↓ BSL
- Palpitations
- Tremor
- Glucagonoma
- ↑ BSL
- Weight loss
- Polyuria
- Gastrinoma
- Zollinger-Ellison syndrome
- Somatostatinoma
- Diabetes
- Cholelithiasis
- Diarrhoea
- VIPoma
- Diarrhoea
- Dehydration
- Hypokalaemia
- Insulinomas
Surgical Stages
- Exposure
- Typically performed by laparotomy
- Laparoscopic and robotic approaches described
- Short gastric vessels ligated
Preserved if spleen-preserving. - Splenic mobilisation
- Splenic artery and splenic vein (at location of pancreatic division) ligated
- Pancreas divided and drained
Preoperative
Assessment:
- Non-specific impact of malignancy
- Cardiorespiratory reserve
- Consider CPET
- Ascites and intravascular volume depletion
- Anaemia correction
- Cardiorespiratory reserve
- Specific effect of malignancy
- Gastric outlet obstruction
- Obstructive jaundice
- Functional tumours
Consultation:
Optimisation:
Premedication:
- Control functional tumours
- Gastrinoma
- High-dose PPI
- Insulinoma
- Consider diazoxide
Cease 24 hours prior to surgery if taking. - Close monitoring of BSL
- Consider diazoxide
- Glucagonoma
- Consider ↑ dose enoxaparin due to risk of VTE
- Gastrinoma
Explain/Consent:
Intraoperative
Preparation:
- Calf compressors
Induction:
Maintenance:
- ↓ Intraoperative fluid administration is suspected to improve pancreatic healing
Echocardiography:
- Use of oesophageal doppler and TOE is described to improve fluid management
Emergence:
Postoperative
Disposition:
Referrals/Review:
Analgesia:
Fluids:
Thromboprophylaxis:
Specific:
- Pancreatic fistula formation
Drain output with amylase >3x ULN of serum amylase concentration. - Diabetes
- Delayed gastric emptying
References
- Jarvis MS, Laing RW, James A. Anaesthesia for pancreatic resection surgery: part 1. BJA Education. 2025 Feb 1;25(2):57–64.
- Jarvis MS, Laing RW, James A. Anaesthesia for pancreatic resection surgery: part 2. BJA Education. 2025 July;25(7):257–64.