Mesenteric Ischaemia
Abdominal surgical emergncy due to interruption of blood supply to the abdominal viscera, which can be classified by aetiology:
- Arterial occlusion
Presentation with abdominal pain and GI symptoms followed by peritonism and shock. Causes include:- Plaque rupture and thrombus
- Arterial embolism
- Venous occlusion
Rare.
- Venous occlusion
- Non-occlusive ischaemia (NOMI)
Severe GI symptoms in the setting of severe circulatory failure, usually with evidence of other organ failures (AKI, ischaemic hepatitis).
Arterial occlusion causes ~50% of cases, and venous occlusion for ~10%.
Epidemiology and Risk Factors
| Arterial Occlusion | Venous Occlusion | Non-Occlusive |
|---|---|---|
|
|
|
Chronic mesenteric ischaemia occurs to atherosclerotic plaque causing partial occlusion of the mesenteric vessels, leading to a form of ‘intestinal angina’ characterised by:
- Post-prandial pain
- Weight loss
- “Food fear”
Pathophysiology
- Arterial occlusion results in ischaemia of a single vascular territory
- Non-occlusive ischaemia results in watershed ischaemia
- Pancreas, between the coeliac and SMA
- Splenic flexure, between the SMA and IMA
The SMA is the most vulnerable to embolic ischaemia due to a higher blood flow rate, larger diameter, and low take-off angle from the abdominal aorta. Emboli classically lodge 3-10cm from the origin of the SMA, and spare the proximal jejunum and colon.
Clinical Features
Diagnosis requires a high level of clinical suspicion.
Features are generally non-specific, aetiology is determined on history and investigations:
The exception is that arterial occlusion typically has an abrupt onset, venous occlusion and NOMI have a more subacute onset.
Pain in NOMI classically id more diffuse and associated with a period of low CO.
- Abdominal pain
Typically severe and out of proportion to the clinical exam findings. - Nausea, vomiting
- Diarrhoea
- PR bleeding
- Peritonism
Late sign, generally indicates irreversible ischaemia and bowel necrosis.
Diagnostic Approach and DDx
Investigations
Blood:
- Lactate
- Metabolic acidosis with ↑ lactate occurs in ~90% of patients
- Lactataemia is not sufficient for diagnosis, but should prompt consideration for CT
Imaging:
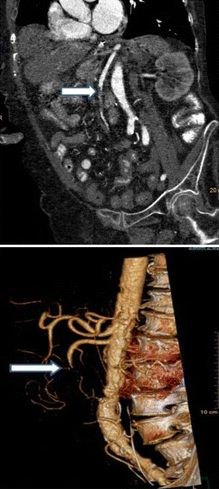
- CT mesenteric angiogram
- Bowel ischaemia
- Portal venous gas
- Intestinal pneumatosis
- Bowel ischaemia
Other:
- Endoscopy
- Visual identification of ischaemia
Management
- Treat shock
- Restore perfusion to ischaemic areas, if possible
- Urgent resection of non-viable bowel prior to perforation
Resuscitation:
- C
- Fluid resuscitation
- Arterial line
- Vasopressors should be used to avoid fluid overload
- Milrinone and dobutamine are preferable
- Correct underlying shock state
- G
- Nasogastric decompression
- Correct concurrent or underlying shock
Specific therapy:
- Pharmacological
- Anticoagulation
For venous ischaemia.- Unfractionated heparin infusion
- Anticoagulation
- Procedural
- Laparotomy
- Mandated for overt peritonitis
- Resect non-viable regions
- Damage control surgery is normal and planned re-look laparotomy within 48 hours is usual
- Restoration of arterial perfusion
- Endovascular
- Stenting
- Catheter-directed thrombolysis or clot retrieval
Can be available for venous or arterial occlusion.
- Open repair (including bypass)
- Endovascular
- Laparotomy
- Physical
Identifying massive gut necrosis should prompt re-evaluation of the appropriateness of curative intent.
Supportive care:
Disposition:
Marginal and Ineffective Therapies
- Intravenous thrombolysis
Successful cases are described, but this is precluded by bowel ischaemia or infarction and so if used must be attempted early.
Anaesthetic Considerations
Complications
- Death
- G
- Short bowel syndrome
After resection. - Perforation
- Short bowel syndrome
Prognosis
Mortality depends intestinal viability, and therefore early diagnosis. In general:
- Occlusive arterial ischaemia has a good prognosis with early detection and aggressive intervention
- Occlusive venous ischaemia has a good prognosis, assuming no bowel necrosis
- The prognosis in NOMI depends on the underlying condition and response to shock
Key Studies
References
- Bersten, A. D., & Handy, J. M. (2018). Oh’s Intensive Care Manual. Elsevier Gezondheidszorg.
- Bala M, Kashuk J, Moore EE, et al. Acute mesenteric ischemia: guidelines of the World Society of Emergency Surgery. World Journal of Emergency Surgery. 2017;12(1):38.