Paracetamol
Paracetamol toxicity causes acute liver injury due to ↑ levels of its toxic metabolite NAPQI due to failure of conjugation with glutathione. This can occur due to either:
- ↑ NAPQI production, exhausting normal glutathione levels
Paracetamol overdose. - ↓ Glutathione levels, ↑ vulnerability to paracetamol in normal doses
Malnutrition.
Epidemiology and Risk Factors
Pathophysiology
Paracetamol is metabolised by two pathways:
- Conjugation with glucuronide sulfates
Normal metabolic pathway (~95% of a therapeutic dose) that produces non-toxic metabolites which are renally cleared. - CYP450 2E1 to NAPQI
- Minor metabolic pathway under normal circumstances
- Produces hepatotoxic NAPQI
- NAPQI is conjugated with hepatic glutathione to non-toxic metabolites which are renally cleared
- Absence of glutathione leads to accumulation of NAPQI
- NAPQI covalently binds multiple proteins, leading to uncoupled oxidative phosphorylation and hepatic cell death
Aetiology
| ↓ Hepatic Glutathione | Cytochrome P450 Induction |
|---|---|
Malnourishment:
|
Antiepileptics:
|
Disease:
|
Other:
|
Clinical Features
Often asymptomatic in the first 24-48 hours; may then develop liver failure.
Gastrointestinal:
- Abdominal pain
- Nausea
- Vomiting
Severe toxicity:
- Coma
- Lactic metabolic acidosis
Assessment
History:
- Dose
- Formulation ingested
- Timing
- Single ingestion
- Staggered ingestion
- Repeated ingestion
Exam:
Investigations
Bedside:
Laboratory:
Imaging:
Other:
Diagnostic Approach and DDx
Management
- Activated charcoal
- NAC
- Liver transplant if fulminant hepatic failure
Resuscitation:
Specific therapy:
- Pharmacological
- Activated charcoal
Appropriate if:- Immediate release within 2 hours
- Modified release within 4 hours
- N-acetylcysteine (NAC)
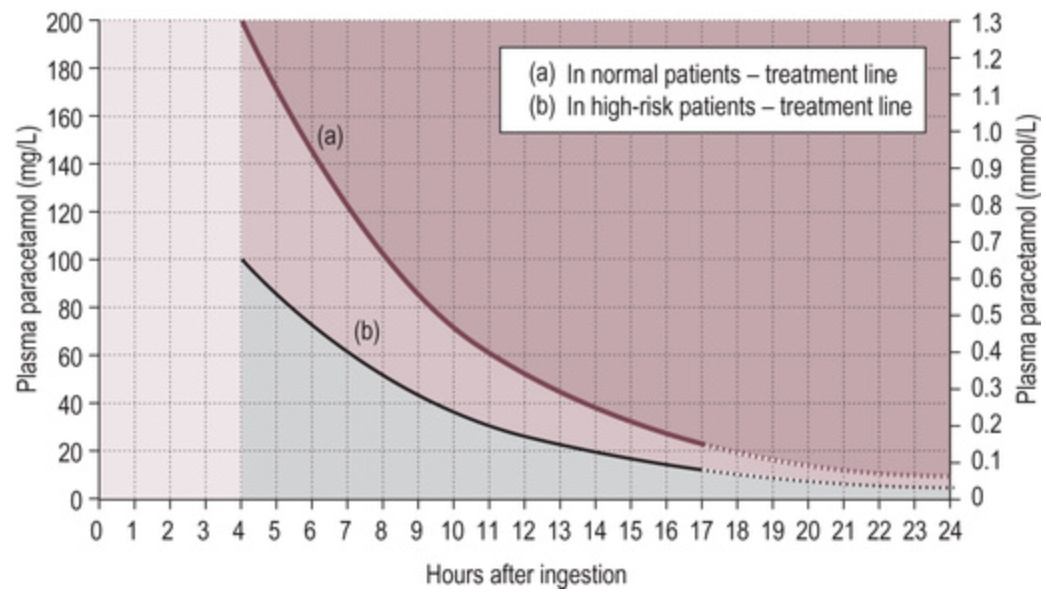
Stimulates glutathione stimulus, allowing NAPQI to be conjugated.- Prescott nomogram indicates when NAC therapy should be given
- >200mg/kg or 10g in a one-off ingestion should receive NAC independent of level
- Inaccurate in sustained-release preparations
Empirical NAC NAC should be given in this circumstance.
- Early administration results in significant reduction in mortality (to <1%), though even late administration may improve outcome.
- 150mg/kg load over 15-60 minutes
- 50mg/kg over 4 hours
- 100mg/kg over 16 hours
- Further doses may be indicated (usually 150mg/kg over 24 hours)
- NAC may be ceased after 24 hours if:
- Paracetamol concentration <10mg/L
- ALT <50U/L
- INR <2
- Clinically well
- Prescott nomogram indicates when NAC therapy should be given
- Activated charcoal
- Procedural
- Liver transplant
Referral indicated for:- SBP <80mmHg
- Hypoglycaemia
- Encephalopathy
- pH <7.3 following resuscitation
- Oliguria
- Creatinine >200μmol/L
- INR >4.5
- INR >3 for 48 hours
- Liver transplant
- Physical
If in doubt, give NAC.
Supportive care:
Disposition:
Marginal and Ineffective Therapies
Anaesthetic Considerations
Complications
Prognosis
Severe hepatic injujry has ~10% mortality.
Key Studies
References
- Bersten, A. D., & Handy, J. M. (2018). Oh’s Intensive Care Manual. Elsevier Gezondheidszorg.