Transversus Abdominis Plane Block
The TAP block is a regional technique to provide analgesia to the anterior abdominal wall, between the mid-clavicular lines. There are three approaches:
- Posterior approach
Performed laterally above the iliac crest, and provides analgesia below the umbilicus. - Subcostal approach
Performed under the costal margin, lateral to the rectus, and provides periumbilical analgesia. - Oblique subcostal approach
Multiple injections along the oblique subcostal line, and provides analgesia to upper abdominal incisions.
Indications
- Abdominal surgery where epidural would be excessive or contraindicated
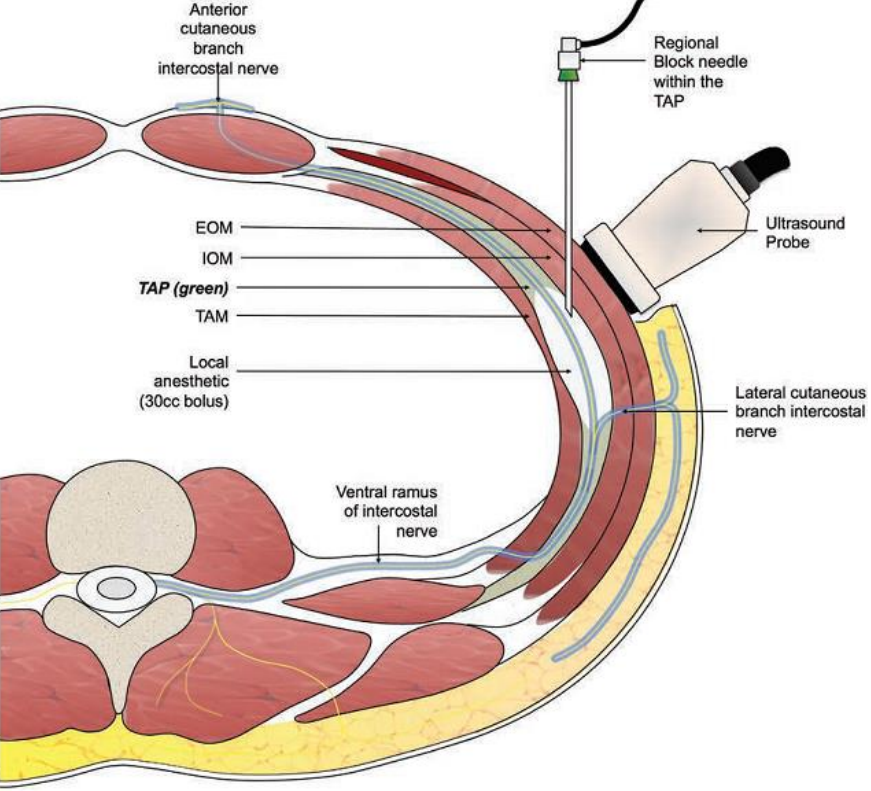
Anatomy
- The TAP lies between:
- Internal oblique and transversus abdominus in the inferior and lateral areas of the abdominal wall
- Rectus abdominus and transversus abdominus in the subcostal abdominal wall
- The TAP contains the thoracolumbar nerves (T6-L1) which innervate the abdominal wall
- Thoracolumbar nerves consist of intercostal, subcostal, iliohypogastric, and ilioinguinal nerves
- All travel beneath the rectus and run for a variable distance through the TAP before penetrating the rectus sheath
This may occur quite laterally, so medial blocks may miss the nerve if it has already penetrated the internal oblique muscle.
Equipment
- Ultrasound machine, gel, probe cover
High or low frequency probe acceptable. - Needle and catheter kit
e.g. 18G Touhy or 21G 100mm ultrasound needle. - Local anaesthetic
Typically 3mg/kg ropivacine (up to 200mg) diluted with N/S to 40ml (20ml each side) - Sterile equipment
Technique
- Prepare equipment
- Identify the rectus abdominus and transversus abdominus muscle at the costal margin

- Scan inferiorly to identify the TAP at the level of the surgical incision
- Place the needle medial to the probe (close to midline), and travel inferolaterally towards the iliac crest into the TAP
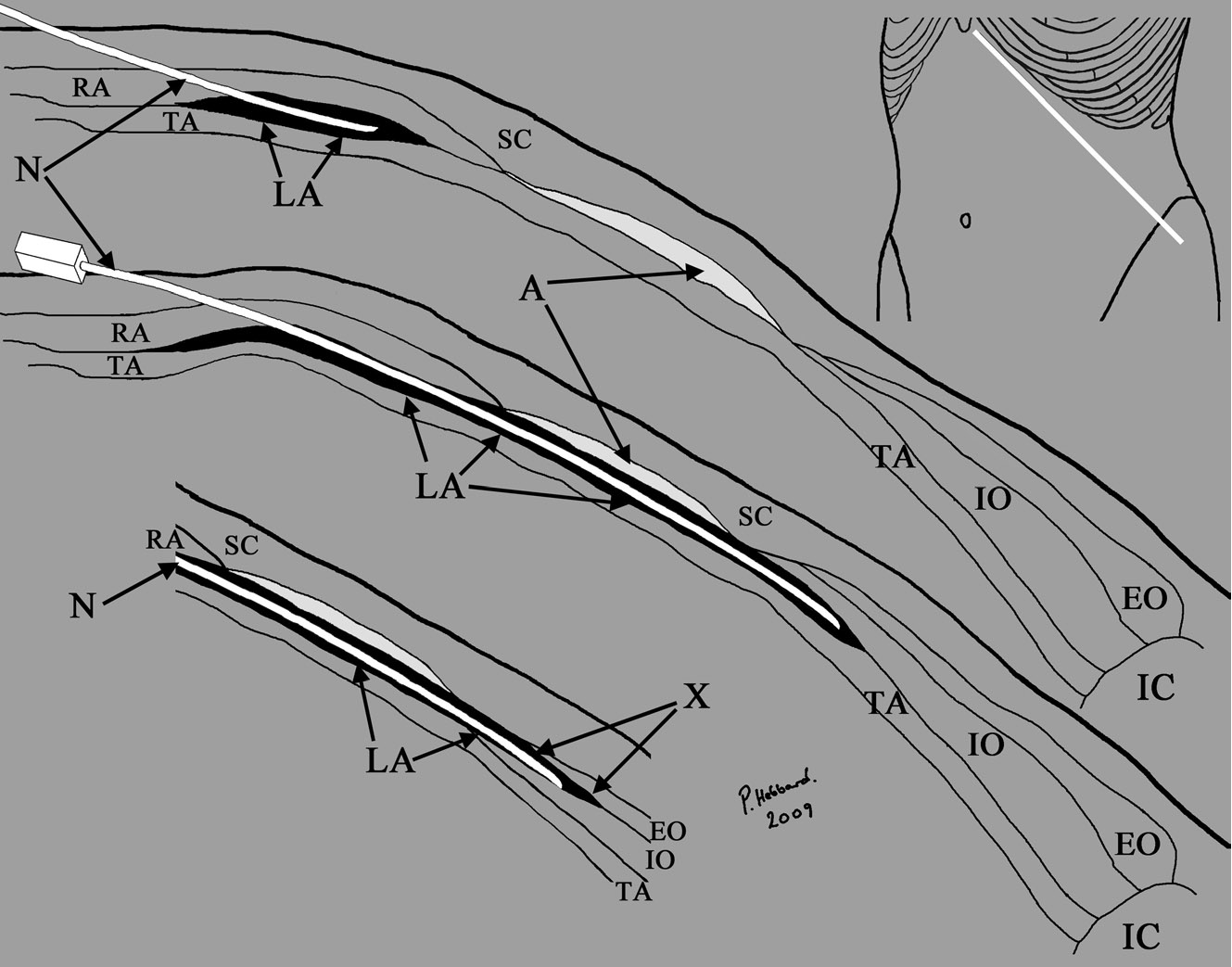
- Hydrodisect the TAP with 1-2ml of LA solution to confirm correct placement
- Wound catheters may also be placed
- Use epidural or nerve block catheters
- Catheters may be left up to 5 days
- Catheters may be managed as:
- Regular boluses (e.g. 20ml of LA solution) Q6H
- Continuous infusion (e.g. 5ml/hr ropivacaine 0.2%)
References
- Hebbard, P. D., Barrington, M. J., & Vasey, C. (2010). Ultrasound-guided continuous oblique subcostal transversus abdominis plane blockade: Description of anatomy and clinical technique. Regional Anesthesia and Pain Medicine, 35(5), 436–441.
- Vincent M, Mathieu O, Nolain P, Menacé C, Khier S. Population pharmacokinetics of levobupivacaine during a transversus abdominis plane block in children. arXiv.